March 2015: Top Challenges 

Peter Davis/Federal Reserve Bank of Boston



{kind=link}
About the Survey
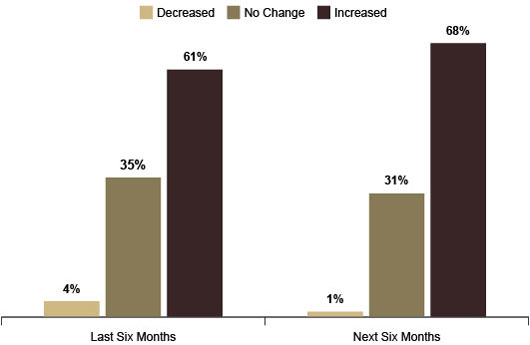
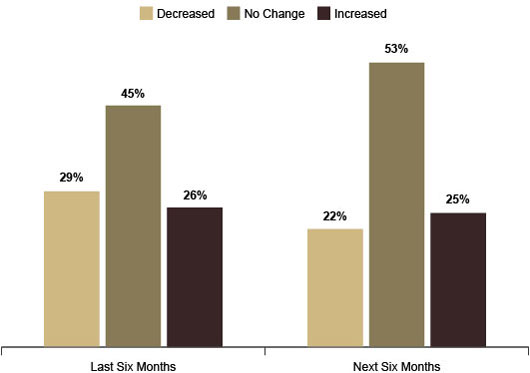
During October 2014, the Federal Reserve Bank of Boston conducted its semiannual New England Community Outlook Survey. As before, the survey covered topics ranging from the availability of credit for small businesses to emerging issues facing lower-income communities. But this time the survey also included three questions on drug and alcohol dependency in respondents' communities. The addition of these three questions was prompted by the written comments of service providers who had responded to the April 2014 survey. Some had written about their concern that drug usage was adversely affecting their communities. Concurrently, alcohol dependency has been addressed in this survey, since many of the issues explored in this report are not confined to only individuals with illicit drug problems but also extend to those with alcohol dependency issues as well. Since the inception of the New England Community Outlook Survey, each iteration has reported an increased demand for services concurrent with funding decreases. In October 2014, current demand and expected future demand for services was on the increase. (Figure 1) For the first time, however, more respondents (25.4%) indicated that they expected funding to increase rather than decrease during the next six months. (Figure 2)
[Compared to five years ago], heroin use is up dramatically as evidenced by a sharp increase in emergency hospital intakes in 2014 v. 2013. This continues to have a detrimental effect on the financial stability of many families and the health of all of our communities. —Survey Respondent
{kind=link}
Figure 1
{kind=link}
Figure 2
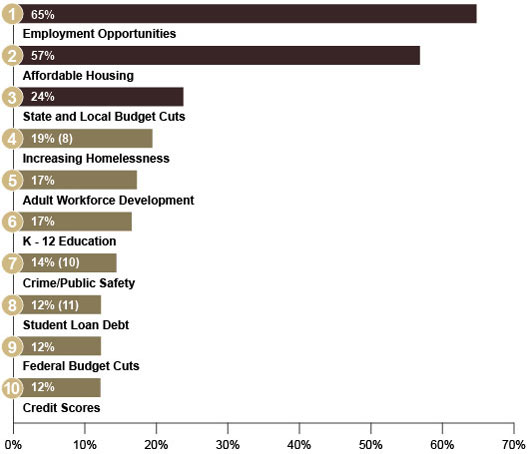
Top Challenges Facing Lower-Income Communities
Survey respondents were asked to rank the top challenges facing lower-income communities. They ranked job availability, access to affordable housing, and state and local budget cuts as the top three challenges. In contrast to results from previous Community Outlook Surveys, federal budget cuts were supplanted by increased homelessness as the fourth greatest challenge.[1] Crime and public safety rose from the No. 10 challenge to No. 7, a change in perception possibly influenced by the increased focus in this survey on drug and alcohol abuse. Included for the first time in the survey as a potential challenge, student loan debt tied with federal budget cuts at No. 8. Since the relaunch of the Community Outlook Survey in 2013, the October 2014 survey results mark the first significant shift in rankings of community challenges, except for the top three challenges — job availability, access to affordable housing, and state and local budget cuts. Drug and alcohol dependency affects every community in New England. Although the efficacy of mitigation efforts varies from community to community, a few of the efforts that states and communities are using to combat drug- and alcohol-related problems will be highlighted in this report.
Increased crime discourages businesses from locating or investing within the city while reducing property values in all sectors. High rates of addiction also impact the labor force and household financial stability. —Survey Respondent
{kind=link}
Figure 3
Drug and Alcohol Dependency in New England
Approximately one in 10 Americans over the age of 12 is a current drug user,[2],[3] and the number of illicit drug users in the United States has grown 26% in the past 10 years. A closer look at the national data reveals that the use of certain drugs is in decline, whereas the use of others has surged during the past decade. For example, nationally, the use of cocaine and inhalants has declined, whereas heroin use has more than doubled. New England has not escaped this surge, experiencing a 20 percent growth in total substance abuse from 2003 to 2012.[4]
Figure 4
Percent Change in Number of Illicit United States Drug Users, 2003 – 2013
|
Substance |
Percent Change |
|
Marijuana |
35% |
|
Cocaine |
-32% |
|
Inhalants |
-13% |
|
Hallucinogens |
28% |
|
Heroin |
143% |
| Prescription Drugs |
2% |
|
Total Percentage Change |
26% |
Sources: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration (SAMHSA). "National Survey on Drug Use and Health, 2013 (ICPSR 35509)." SAMHSA. "National Survey on Drug Use and Health, 2003."
In October 2014, New England Community Outlook Survey participants were asked the following three questions related to drug and alcohol dependency:
- How has drug and alcohol dependency changed in the communities you serve?
- What is the impact of the change in your communities?
- What are some of the perceived characteristics of drug- and alcohol-dependent individuals who live in your community?
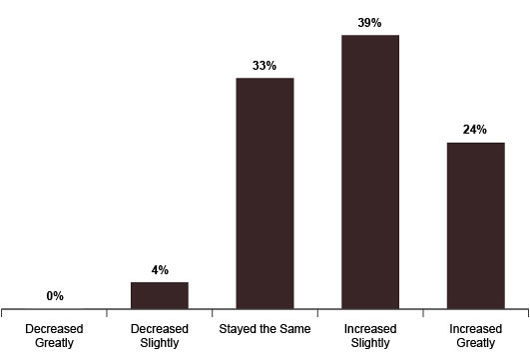
Reflecting national trends, 63% of respondents reported an increase in drug and alcohol dependency in their communities, whereas less than 4% reported a decrease. (Figure 5)
{kind=link}
Figure 5
{kind=link}
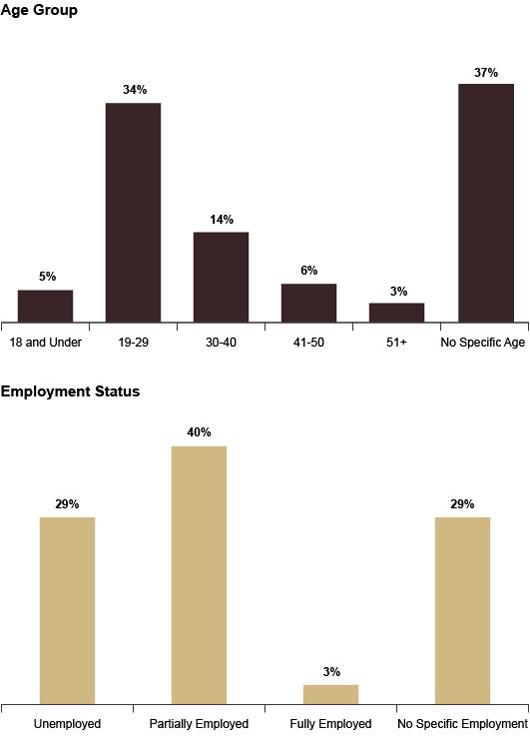
Figure 6
Survey respondents reported that 69% of those characterized as drug and alcohol dependent individuals ranged in age from 19 to 29 years old and were unemployed or partially employed. In contrast, five survey recipients reported that a majority of drug- and alcohol-dependent individuals in their communities were over 50 years old.
New England's War on Substance Abuse: The Northern Front
"During the tenure of every governor there are numerous crises. Some are created by natural disasters when we all need to pull together to provide immediate relief
from pain and heartbreak. …There are other crises that confront us that are actually much tougher because they are more complicated, controversial, and
difficult to talk about. …The crisis I am talking about is the rising tide of drug addiction and drug-related crime spreading across Vermont."
—Governor Peter Shumlin of Vermont
On January 7, 2014 Governor Peter Shumlin of Vermont dedicated his entire State of the State message to the drug addiction issue that continues to destabilize so many communities across New England. He urged policymakers, educators, healthcare workers and law enforcement personnel to view the recent surge in substance abuse as a barrier to local economic development and as a public health crisis, a sharp contrast to the traditional criminal justice frame.[5] Governor Shumlin had shone a spotlight on the battle Vermont is fighting against a trifecta of illicit substances: marijuana, diverted prescription pain relievers, and heroin (among other opiates). Although drug abuse epidemics have been historically an "urban problem," the nature of the market and the demographic profiles of users have changed in ways that are particularly threatening to the economic well-being of New England's northern tier states (New Hampshire, Vermont, and Maine), which are characterized by vast rural areas as well as aging and shrinking populations. A 2014 PolEcon Report, The Corrosive Effects of Alcohol and Drug Misuse on NH's Workforce and Economy, estimates that this issue cost the state more than $1.84 billion in 2012 due to "lost worker productivity and earnings, [along with] increased expenditures for healthcare and public safety [services][6] ". At the local level, New Hampshire's municipalities spend about 16 percent of their budgets on drug abuse and addiction issues, making it the second largest expenditure (after education) on their books[7].
Drug and Alcohol Consumption Trends in the Northern Tier States
The aim of the following section of this Community Outlook Survey report is threefold:
(1) To briefly analyze the key trends in drug and alcohol use in New Hampshire, Maine, and Vermont and to highlight the demographics of high-risk users in these states.[8]
(2) To provide one example of a promising cross-sector, community-based, and data-driven approach to substance abuse reduction.
(3) To outline the significant challenges facing practitioners and local coalitions working on prevention, intervention, and treatment projects.
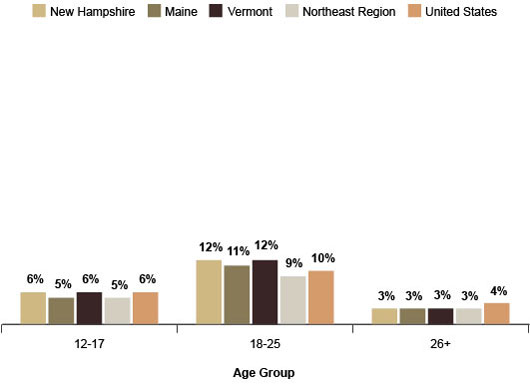
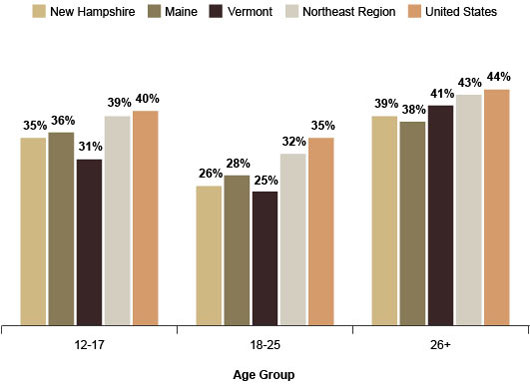
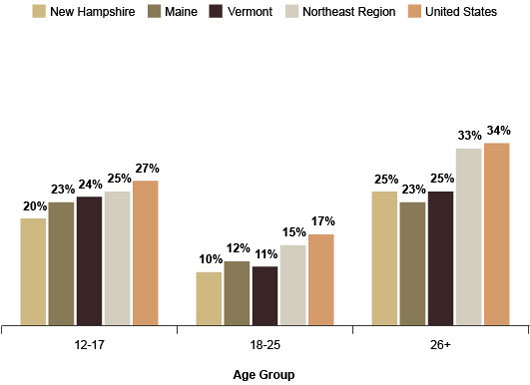
Which social groups face the greatest risk of alcohol and drug use/abuse?[9] In preparation for this report, we contacted several practitioners in Vermont, New Hampshire, and Maine whose jobs allow them to interact directly with alcohol- and drug-dependent individuals. [10] We heard repeatedly in our interviews with local practitioners that in the northern tier states today's drug addiction issue transcends all income levels, gender, racial or ethnic differences, as well as rural/suburban/urban distinctions.[11] However, a person's likelihood to binge drink or use illicit drugs differs significantly by age category.[12] In New Hampshire, Maine, and Vermont, for every major substance type young adults (18–25 years old) exhibit higher rates of substance consumption than youth populations (12–17 years old) and adult populations (older than 26 years of age). While alcohol and marijuana continue to account for the highest number of users across all age cohorts, nonmedical use of prescription drugs (particularly opiates) and heroin is a growing concern for treatment providers because the number of people seeking help with opiate and heroin addiction has nearly tripled since 2004.[13] In contrast to the 1970s stereotype of the unemployed, inner city addict, more than 75 percent of current users participate in the workforce in Maine.[14] Data on workforce participation in other states was limited but only 29% of respondents to the Community Outlook Survey felt that the majority of drug- and alcohol-dependent individuals were unemployed.
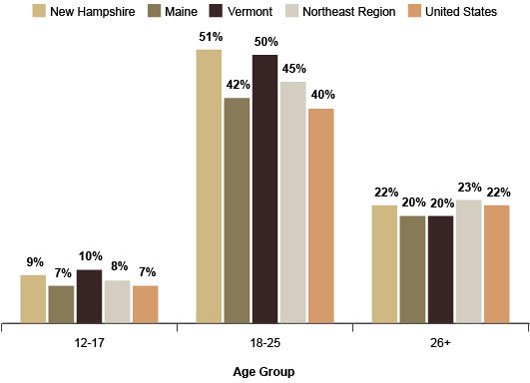
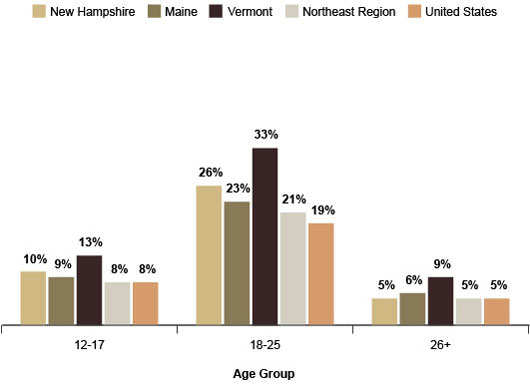
According to the most recent state-level data from the National Survey on Drug Use and Health, New Hampshire and Vermont stand out as having statistically higher rates of binge drinking, marijuana use, and prescription drug use among all age categories as compared to the national averages. For instance, more than 50 percent of young adults in New Hampshire engage in regular binge drinking, while less than 40 percent of their counterparts do so across the nation. Interestingly, Maine's figures for binge drinking and prescription pain relievers mirror the national averages, but its residents' marijuana use rates are among the highest in the country. Almost 3 out of every 10 respondents in the 18–25 age group reported smoking marijuana at least once in the past month. Young adults in the 18–25 age group are more likely to use and abuse each of the aforementioned substances. (Figure 7, Figure 8, Figure 9)[15]
{kind=link}
Figure 7
{kind=link}
Figure 8
{kind=link}
Figure 9
According to Sheldon Wheeler, acting director of Maine's Office of Substance Abuse and Mental Health Services, a key contributing factor to the state's high proportion of marijuana users is the dangerously low perception of harm from regular use. Among the youth demographic, the majority of participants in the 2009–2011 Maine Integrated Youth Health Surveys replied that they "felt there was little to moderate risk of harm involved"[16] in smoking marijuana. This figure was more than 10 percentage points higher for young adults (18–25 age group). Wheeler emphasized the fact that many parents in communities where he visits wrongly assume that the marijuana encountered by kids today is identical in potency to the marijuana sold three decades ago. According to national data from confiscated cannabis samples, the average THC content of marijuana has increased from 1.37 percent in 1978 to 8.49 percent in 2008.[17]
The perception of binge drinking and marijuana use is statistically higher in the northern tier states for all age categories as compared to the national averages. (Figure 10, Figure 11)
{kind=link}
Figure 10
{kind=link}
Figure 11
Comparing reports for 2007 and 2012, National Survey on Drug Use and Health statistics for alcohol, marijuana, prescription painkillers (particularly opiates), and heroin reveal the following key trends:
- A reduction in the share of binge drinkers among youth (12–17 years old) in the northern tier states, as well as a reduction in the rates for the older respondent groups (over the age of 26).[18]
- Increased rates of marijuana use for all age groups in New Hampshire and Vermont. In Maine, a decrease in marijuana use overall among youth and young adults but an increase in adults over 26 years of age.[19]
- A general decrease in the misuse of prescription medication among all groups possibly due to enhanced statewide regulation and monitoring of prescribed pain relievers.
Drug and alcohol dependency is frequently cited as a workforce concern. Ours is a lower income community, and yet our manufacturers cannot fill many open positions. —Survey Respondent
Complex Solutions for a Complex Problem
For northern tier states, where between 35 and 60 percent of people live in rural areas,[20] the drug addiction issue threatening their communities appears "larger than life." Practitioners working to reduce substance abuse rates among affected populations know all too well that this epidemic is an outcome of complex social and economic problems that affect sectors, including law enforcement, education, business, and the healthcare industry. While local and national media have written extensively about northern tier drug problems, much less attention has been focused on promising community-based initiatives that emerged throughout this geography to tackle the substance abuse crisis in a comprehensive way.
Formed in 2007, New Hampshire's North Country Regional Network (NCRN) effort illustrates how a diverse group of community stakeholders from key sectors can join forces to leverage existing resources and local expertise in order to design evidence-based approaches that achieve results. Located in the northernmost, sparsely populated, and poorest part of New Hampshire, the NCRN provides insights into the existing challenges and structural limitations impeding efforts to reach the population-level goals for reduction of drug dependency.[21]
Cross-sector collaboration or collective impact models are not new tools in the field.[22] But the NCRN has adapted such approaches to a rural geography and has experimented with connecting six hyperlocal community collaboratives into a functional network to achieve regional-level goals. Another notable aspect of this network is that it has been part of the state government's intervention to address New Hampshire's dismal drug abuse statistics. Believing that cross-sector and interagency collaboration was essential at both the state and local levels, the Governor's Commission on Alcohol and Drug Abuse Prevention, Treatment, and Recovery created 10 regional networks across the state to convene local coalitions and provide them with key resources to develop prevention strategies tailored to specific community contexts.[23]
The state's sponsorship of North Country Health Consortium, a prominent organization in the region, to act as convener and fiscal agent helped community members take ownership of this initiative and customize the organizational structure of the effort to add Community Action Teams as liaisons for the six geographically isolated residential nodes. After several years of community organizing, and collecting and reviewing local and county-level data on drug and alcohol abuse trends, the NCRN produced a Strategic Action Plan for 2012–2015 that detailed their interventions to mitigate the most pressing issues for the population: alcohol, marijuana, and prescription drug misuse by teenage youth in the region. While the initiative design phase was process-heavy, the NCRN achieved a high level of community engagement and forged connections between schools, law enforcement, businesses, healthcare professionals, parents, and kids. Although the regional network is still in its nascent phase, it has already produced some important lessons:
- Good local data (at the neighborhood or town level) has been collected on substance abuse among different populations. There were variations in drug and alcohol consumption trends among schools in the six residential hubs, suggesting that rural environments are not a monolith. Emerging strategies need to account for such nuances.
- It is important to place students in leadership positions in the coalitions and to provide them with support to lead prevention-related efforts in their own schools. Superintendents of local high schools have also been critical players in the collaborative by offering in-kind support for many of the network's prevention activities and survey data collection.
- Parts of the NCRN, such as the Connecticut Valley, experienced greater problems with diverted prescription drugs due to sharing a border with Vermont. Cross-state collaboration among the Valley's primary care doctors, treatment providers, pharmacists, and law enforcement agencies was essential to reversing trends. After convening a Community Summit on Diverted Prescription Drugs in 2011, 76 attending practitioners from New Hampshire and Vermont committed to adopting a number of independent action steps to help mitigate the risk of medication misuse by their patients.[24]
While the overall success of the regional network initiative will undergo formal evaluation during the coming years, some of its challenges are already evident. The precariousness of funding streams from state and federal governments and local philanthropy will determine how much of the planned activities become operationalized. Another significant limitation of this strategy is its exclusive focus on the teenage population, even though the drug abuse issue is more severe for the 18- to 25-year-old group[25]. Teenagers can be reached through a partnership with schools. But a deeper engagement with local employers may offer access to young adults.
Conclusion
The high levels of drug and alcohol abuse among younger residents in New England is a devastating force that strains communities in complex ways. It directly affects a number of the top challenges our survey participants highlighted for lower-income populations. The single greatest cost of substance abuse (about 63 percent) is reduction in worker productivity[26]. A growing proportion of substance users in the workforce not only reduces an employer's revenue, but it discourages new businesses and jobs from committing to areas where substance abuse is a challenge. The reported rise in homelessness and public safety concerns reflected in the October 2014 New England Community Outlook Survey may be exacerbated by the opiate and heroin epidemic that erodes users' financial well-being and drives many individuals into a life of crime.
New England's northern tier states, with a large share of under-resourced rural and small town populations, are particularly concerned about the impact drug and alcohol addiction have on their youth and young adults who will become tomorrow's workers, parents, and community builders.
The scope and urgency of the problem echoed in Vermont Peter Governor Shumlin's State of the State message has pushed Vermont, Maine, and New Hampshire to think about putting into action community-based strategies to decrease and prevent substance abuse in their geographies. Cross-sector collaborations between government, law enforcement, healthcare, education, and business sectors have become a salient element of state and local initiatives that strive to build healthy places to live and work.
New England's community development challenges benefit from the experience, knowledge and motivation of community organizations working within our region every day. While this report tried to shine some light on one of the concerns—substance abuse—providers throughout the area simultaneously are addressing other critical issues like affordable housing and quality education.
The New England Community Outlook Survey will continue to ask service providers for local knowledge about how lower-income communities are faring and how the Federal Reserve Bank of Boston can provide insight on these issues.
"Northern New England has a clear and apparent crisis on its hands. The opiate epidemic will continue to ravage communities—economically and otherwise—until we can come up with a serious plan to push back the wave of addiction. Vermont's governor has made the issue a core component of his platform. It's past time for the other states to follow suit and to come up with a comprehensive, regional plan to tackle the issue."
—Survey Respondent
[Drug and alcohol dependency is] causing a crisis of sorts for entry-level jobs. Applications are down as folks are avoiding drug screenings. The jobs that are filled have a large amount of turnover because of problems with the workforce that, many times, tie directly to drug abuse. —Survey Respondent
Methodology
For the past two years, the Federal Reserve Bank of Boston has conducted the New England Community Outlook Survey. The respondents represent organizations providing direct services to lower-income households. Organizations are asked twice a year to designate a senior staff member to respond to the six-minute survey. For the latest iteration of the survey, 160 service providers from the economic development, affordable housing, community action, human services, and workforce development sectors in each of the six New England states responded to 24 multiple-choice and fill-in questions. We asked respondents to comment on the changes in conditions over the previous six months and to project changes over the next six months. Respondents completed the survey between October 14, 2014 and November 10, 2014.
Data collected represent the opinions of service providers who completed the survey. While we strive to include a reasonably representative sample in our survey, responses should not be interpreted to represent the opinions of all service providers in New England.

 About the Authors
About the Authors
Anthony S Poore
Kseniya Benderskaya
Kaili Mauricio
Endnotes
- This shift in ranking cannot be attributed to an overweighted response from the affordable housing sector, because this iteration of the survey registered a decrease in that sector's survey response from 36 percent in April 2014 to 31 percent in October 2014. Thus, a higher response rate among housing-related service providers was not responsible for homelessness rising to become the No. 4 challenge.
- Substance Abuse and Mental Health Services Administration, Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-48, HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
- According to the Substance Abuse and Mental Health Services Administration, a current drug user is one who, at the time of the survey, had used illicit drugs in the previous 30 days.
- Substance Abuse and Mental Health Services Administration (SAMHSA). "Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings." Rockville, MD: SAMHSA, 2013.
- Seelye, K.Q. "In Annual Speech Vermont Governor Shifts Focus on Drug Abuse." New York Times, Jan. 8, 2014 (located at: http://www.nytimes.com/2014/01/09/us/in-annual-speech-vermont-governor-shifts-focus-to-drug-abuse.html?_r=0).
- PoleEcon Research. "The Corrosive Effects of Alcohol and Drug Misuse on NH's Workforce and Economy." Nov. 2014 (located at http://www.new-futures.org/sites/default/files/Summary%20Report_0.pdf).
- North Country Regional Network: Strategic Plan for Prevention 2012-2015. (located at http://www.nhcenterforexcellence.org/pdfs/strategicplans/NorthCountrySP_Final.pdf).
- We chose to analyze New Hampshire, Maine, and Vermont because service providers from the three northern New England states had written more frequently on past Community Outlook Surveys about their concerns related to substance abuse issues.
- No nationwide surveys exist that report on illicit drug consumption at the national, state and county levels; only data for alcohol use has been collected. As a result our current analysis relies on each state's records of admission to public treatment facilities, as well as other locally collected data to paint the demographic profiles of current users. Missing from all existing sources of information are people's income data, census tract or city of residence, occupation, and employment status. To fill in these gaps, the authors interviewed a number of professionals in the substance abuse treatment field in each of the three states and used anecdotal evidence to supplement current data limitations.
- While some practitioners interviewed in this phase of our data collection had been respondents to the October 2014 New England Community Outlook Survey, most of the people we contacted were not.
- Interview on December 4, 2014 with Sheldon Wheeler, acting director of the Maine Office of Substance Abuse and Mental Health Services; interview with Lisa Muré, M.Ed, CPS, Director/Project Manager for Prevention at New Hampshire Center for Excellence; interview on November 26, 2014 with Geoffrey Miller, Associate Director for Prevention and Intervention Services at Maine Office of Substance Abuse and Mental Health Services , Interview on November 7, 2014 with Linda Paquette, executive director at New Futures; and on December 5, 2014 with Stacey Chandler, Data Specialist, Data & Research Team.
- 2003-2012 National Survey on Drug Use and Health.
- Compilation of data from the New Hampshire Bureau of Drug and Alcohol Services, the Vermont Department of Health's Division of Alcohol and Drug Abuse Programs, and the Maine Office of Substance Abuse Treatment Data System.
- Maine Department of Labor Substance Abuse Testing Law (http://www.maine.gov/labor/labor_laws/substance_abuse_testing/ ) and the Maine Substance Abuse Testing Report (located at http://www.maine.gov/labor/labor_stats/publications/substanceabuse/index.html).
- Northeast region refers to the United States Census region, which includes the New England States as well as Pennsylvania and New York.
- Hornby Zeller Associates, Inc. "Substance Abuse Trends in Maine: State Epidemiological Profile 2013." April 2013 . (located at http://www.maine.gov/dhhs/samhs/osa/pubs/data/2013/SEOWEpiProfile2013FINAL.pdf).
- National Institute on Drug Abuse. "Quarterly Report Potency Monitoring Project." March 2009 (located at https://www.ncjrs.gov/pdffiles1/ondcp/mpmp_report_104.pdf).
- Substance Abuse and Mental Health Services Administration (SAMHSA), National Survey on Drug Use and Health, 2012 (ICPSR 34933). SAMHSA, "National Survey on Drug Use and Health, 2007 (ICPSR 23782)."
- Substance Abuse and Mental Health Services Administration (SAMHSA), National Survey on Drug Use and Health, 2012 (ICPSR 34933). SAMHSA, "National Survey on Drug Use and Health, 2007 (ICPSR 23782)."
- U.S. Census Bureau, 2010-2012 American Community Survey 3-Year Estimates: Selected Demographic Characteristics.
- "North Country Regional Network: Strategic Plan for Prevention 2012–2015" (located at http://www.nhcenterforexcellence.org/pdfs/strategicplans/NorthCountrySP_Final.pdf).
- Collective impact models focus on the cooperation of individuals or organizations across different sectors towards a specific goal.
- New Hampshire Bureau of Drug and Alcohol Services, "New Hampshire's System for Substance Abuse Prevention Efforts and Services" (located at http://web.cof.org/2013fall/docs/resources/NHOAD_PrevSummaryOnline_9.19.13.pdf).
- "Upper Valley Summit on Diverted Prescription Drugs," September 2011 (located at http://www.nhcenterforexcellence.org/pdfs/strategicplans/UValleyCmmtySummit_RxDrugs.pdf).
- NH Bureau for Drug and Alcohol Services and NH Center for Excellence. "Community Data Profile: North Country Region." August 2011 (Located at http://www.nhcenterforexcellence.org/pdfs/dataprofiles/North_Country_Region_complete.pdf).
- PoleEcon Research. "The Corrosive Effects of Alcohol and Drug Misuse on NH's Workforce and Economy." Nov. 2014 (located at http://www.newfutures.org/sites/default/files/The Corrosive Effects of Alcohol and Drug Misuse on NH's Workforce and Economy_4.pdf).