Drugs, Death, and Despair in New England 

Sezeryadigar/iStock
The opioid crisis has been called a national epidemic. In New England it blights urban, suburban, and rural communities, fueled by prescription pain killers and cheap and plentiful heroin.



{kind=link}
To say that the United States is in the midst of an opioid epidemic seems almost cliché at this point. Over the past two years, thousands of articles have been written about the crisis; nearly all US states and counties have held public hearings, town halls, and symposia; Congress passed the Comprehensive Addiction and Recovery Act of 2016; and President Obama pledged funding and action to address the crisis.
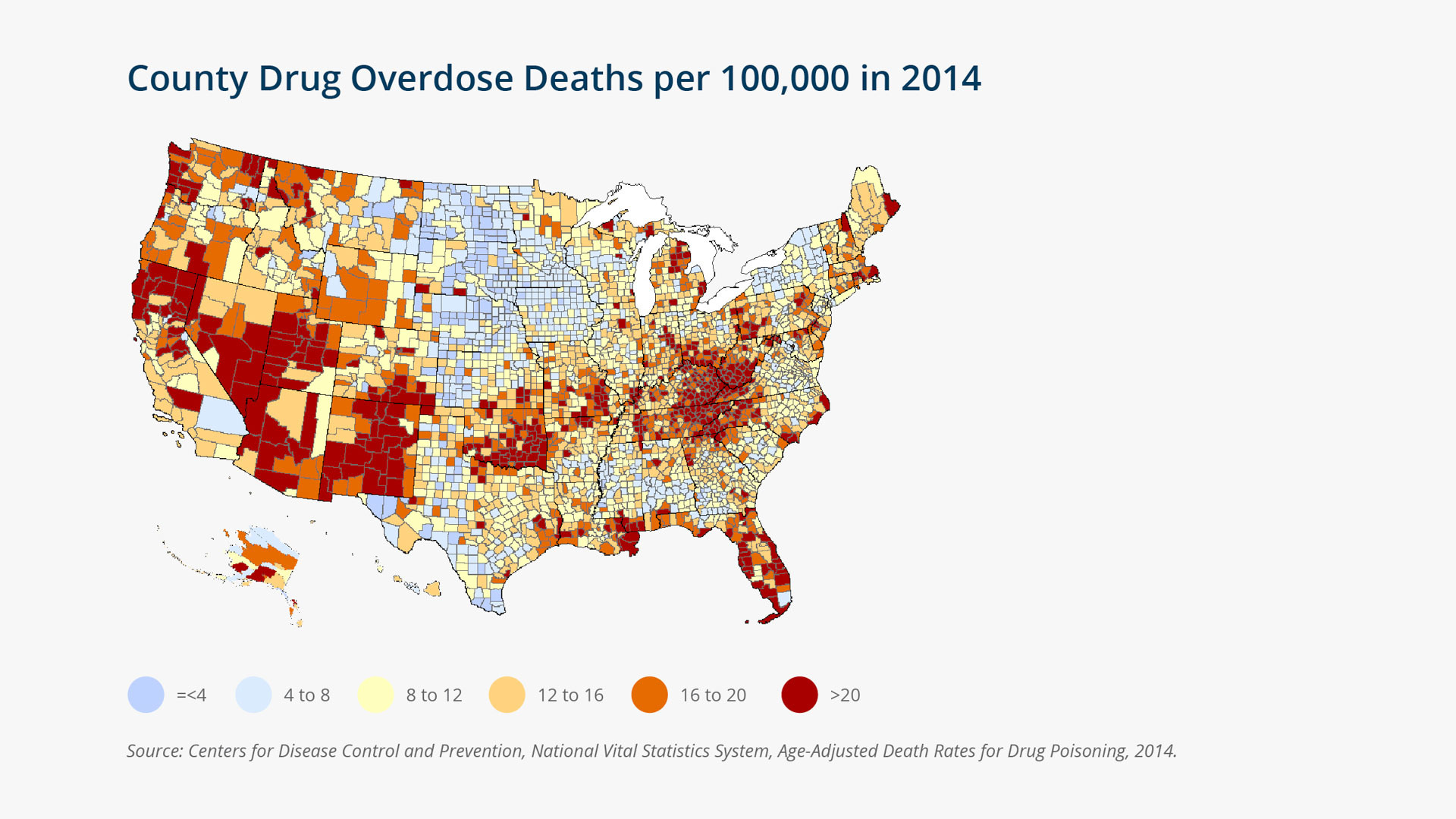
Most media commentary has characterized the crisis as a national epidemic. That portrayal is accurate. The US overdose death rate reached 15 per 100,000 in 2014 and is climbing at a much faster rate than other causes of death, due primarily to opioids (prescription pain relievers and heroin).1 Opioids now kill more Americans than do motor vehicle accidents. In 2014, 28,647 (61 percent) of drug overdose deaths involved an opioid, and nearly all counties in the United States experienced increases in drug overdose mortality over the past decade. (See "County Drug Overdose Deaths per 100,000 in 2014.")
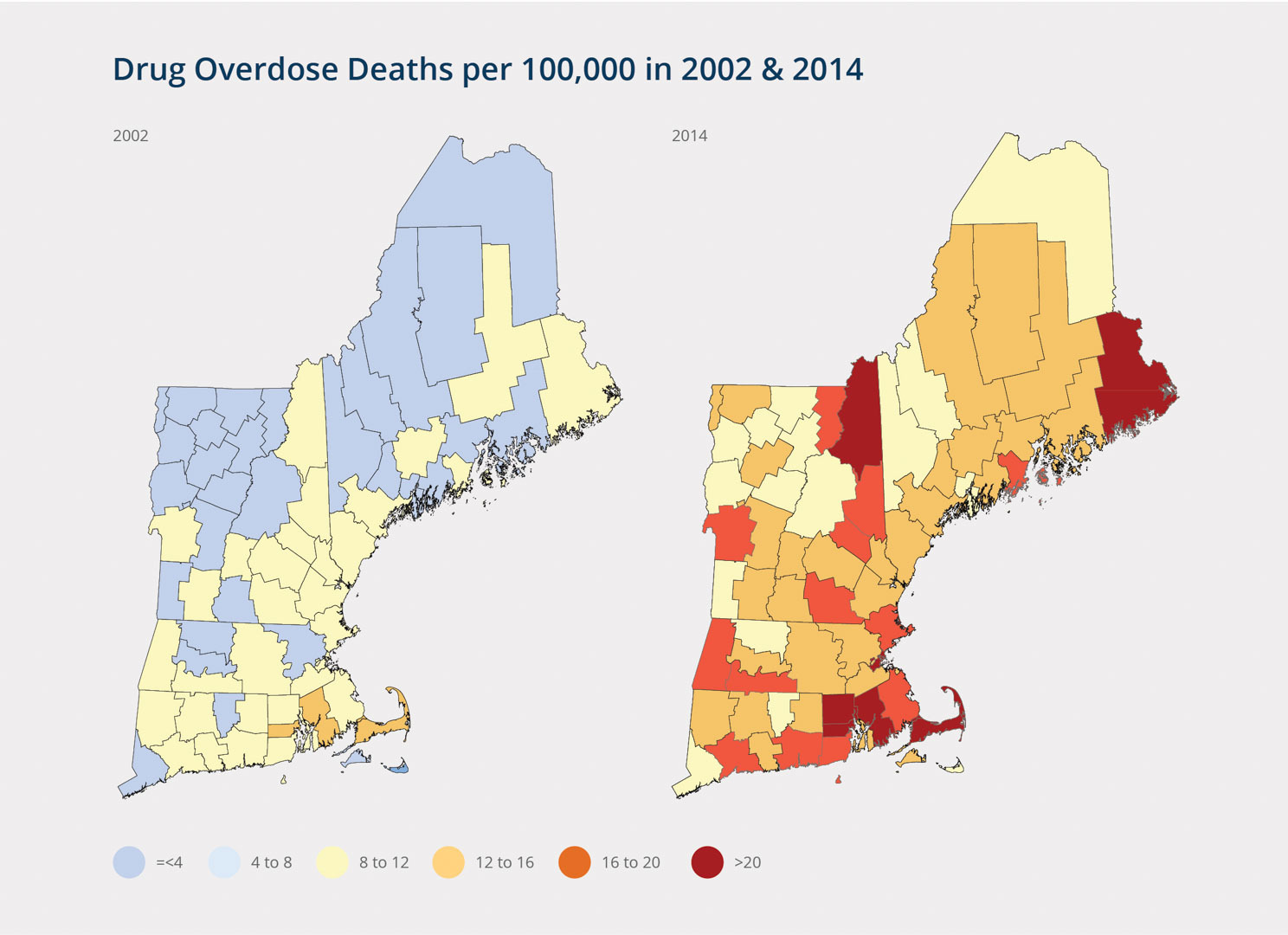
High overdose mortality rates were once mostly restricted to large cities and Appalachia. Now, however, places considered buffered from widespread drug problems as recently as a decade ago, including New England, face surging drug overdose mortality rates. Between 2002 and 2014, drug overdose mortality rates more than doubled in every New England county. Washington County, Maine; Barnstable, Bristol, and Suffolk counties in Massachusetts; Coös County, New Hampshire; and Kent and Providence counties in Rhode Island now have drug overdose mortality rates above 20. (See "Overdose Deaths per 100,000 for New England Counties in 2002 and 2014.")
The highest overdose mortality rates in New England span the rural-urban continuum, including places as urban as New Haven County, Connecticut, and places as sparsely populated as Essex County, Vermont—the least populated county in New England. Still, the 20 New England counties that had overdose mortality rates above 16 in 2014 have several characteristics in common, including poverty, disability, unemployment rates that exceed New England averages, and above-average declines in manufacturing and manual-labor occupations since 1970.
{kind=link}
Rachel Bissett/Federal Reserve Bank of Boston
Adolescent Drug Abuse and Overdose
Nationally, overdose rates are highest among individuals aged 25 to 54, but adolescents and young adults also abuse and overdose. In 2014, the overdose death rate among individuals aged 15 to 24 was 8.6, with the highest rate among non-Hispanic white males (17.4), followed by non-Hispanic white females (7.0), Hispanic males (6.0), black males (4.0), Hispanic females (2.5), and black females (2.3).2
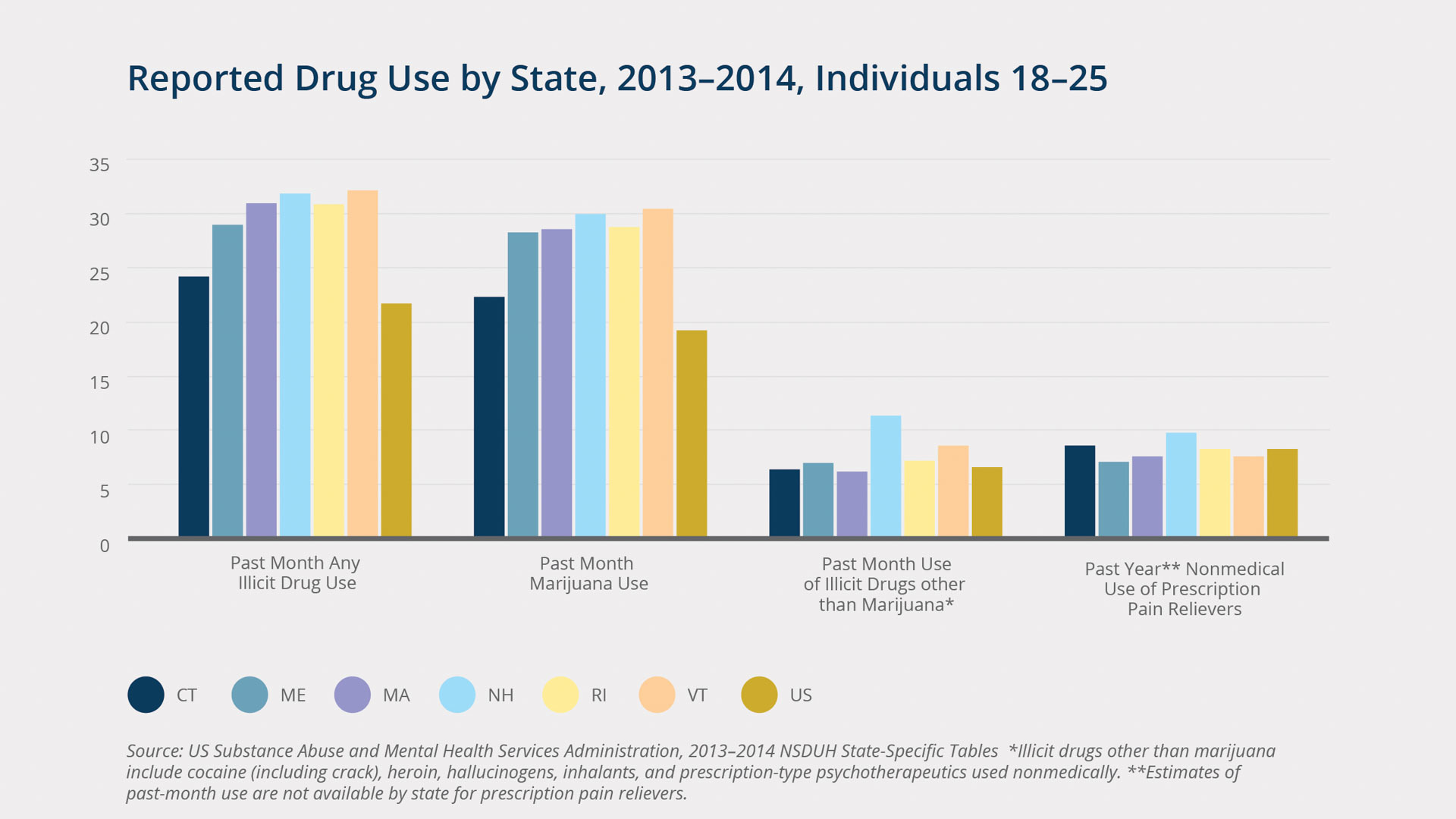
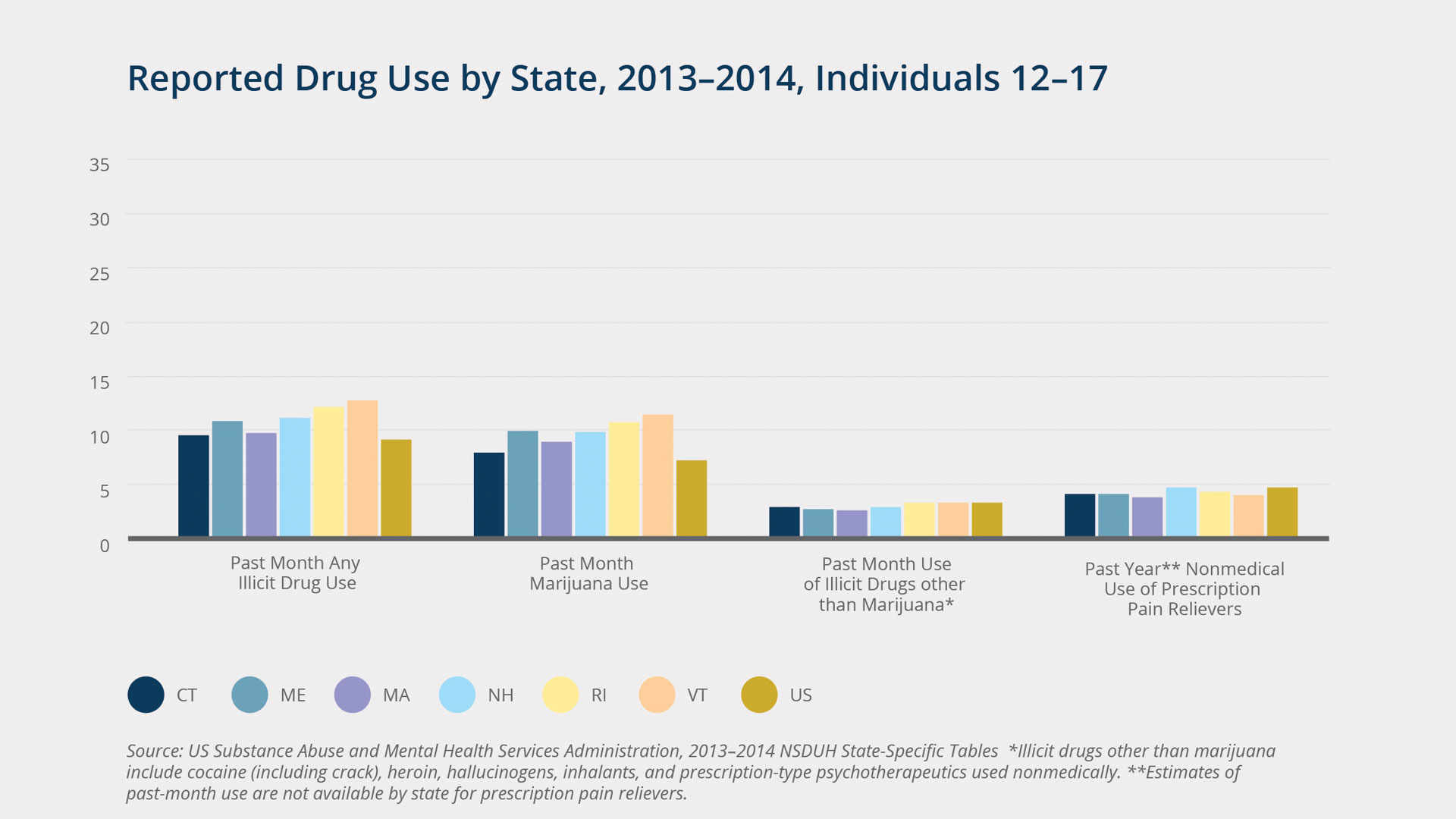
As noted earlier, the surge in overdose mortality has been driven by prescription pain relievers (e.g., oxycodone, hydrocodone) and heroin. Although rates of abuse are much higher among young adults (18–25), over 1.1 million adolescents (4.7 percent of youth aged 12–17) abused prescription pain relievers in 2014.3 Among both teens and adults, only marijuana is more frequently abused than prescription pain relievers.4 See "Reported Drug Use by State, 2013–2014, Individuals 12–17" and "Reported Drug Use by State, 2013–2014, Individuals 18–25." Adolescent drug use is particularly worrisome because this is the period when most substance abuse and addiction disorders begin, and abuse during these formative years increases the likelihood of future economic precariousness, relationship instability, poor health, and criminal-justice involvement.
Rates of current (past-month) illicit-drug use among adolescents and young adults are higher in all New England states than in the United States overall.5 However, overall illicit-drug use rates are driven mostly by marijuana. Although there are short- and long-term adverse effects associated with marijuana use, there have been no reported overdose deaths from marijuana. Nonmedical use of prescription opioids, while much less prevalent, is unequivocally much more deadly. Adolescent abuse of prescription pain relievers in New England is comparable to the overall US rate. However, among young adults (aged 18–25), rates of nonmedical use of prescription opioids are higher in Connecticut and New Hampshire than in the United States overall.
Using data from the National Survey on Drug Use and Health, my colleague and I found that the most salient contributors to opioid abuse among adolescents and young adults are poor mental health, peer substance use, the perception that substance use is not risky, and having access to drugs.6 Adolescents who smoke daily and consume alcohol to excess are more likely than their nonsmoking and nondrinking peers to use illicit drugs and to abuse prescription opioids. Importantly, use of emergency departments, where opioids are more commonly prescribed, also increases adolescents' risk of abusing opioids.
{kind=link}
Rachel Bissett/Federal Reserve Bank of Boston
How Did We Get Here?
US overdose deaths involving prescription opioids have quadrupled since 1999. Not coincidentally, so have sales of prescription opioids. Annual sales of OxyContin (a brand name for the drug oxycodone)—the most widely prescribed, abused, and profitable prescription narcotic in history—alone skyrocketed from $45 million in 1996 (when it entered the market) to $3.1 billion by 2010. In Dreamland: The True Tale of America's Opiate Epidemic, Sam Quinones notes that Purdue Pharma, the company that makes OxyContin, aggressively marketed its blockbuster drug for chronic noncancer pain, particularly in areas with relatively high shares of blue-collar laborers who were at risk of work-related back pain and other injuries.7 In 2007, Purdue Pharma and three of the company's executives pleaded guilty in federal court to criminal charges that they misled regulators, physicians, and patients about OxyContin's addiction and abuse potential. However, by then, 5.2 million Americans were already misusing prescription opioids,8 and annual prescription opioid–related overdose deaths exceeded 14,000.9
Over the past decade, public-health and government efforts have focused on combating the prescription opioid epidemic by cracking down on "pill mills" (medical establishments that prescribe pills inappropriately), creating statewide prescription-drug monitoring programs, and educating physicians on safe prescribing practices. These efforts have been largely successful; there have been recent declines in prescription opioid abuse and overdose deaths among both adolescents and adults.10 However, there has been an unintended consequence. As the supply of prescription opioids has dwindled, heroin, which produces the same high and is just as addictive, has filled the gap. About 80 percent of people who are currently using heroin report misusing prescription opioids first.11 Increased mixing of heroin with the synthetic pain reliever fentanyl (which is up to 50 times more powerful than heroin) has made New England's opiate problem much more deadly.
{kind=link}
Rachel Bissett/Federal Reserve Bank of Boston
Moreover, despite widespread awareness of prescription opioid abuse, high rates of opioid prescribing continue, though they vary by state.12 Maine currently ranks first and New Hampshire ranks third in the nation in prescribing rates for long-acting/extended-release opioids, which have an especially high overdose risk because abusers can crush them and instantly achieve the full dose (possible even with so-called abuse-deterrent formulations). Massachusetts (8th), Connecticut (13th), Rhode Island (14th), and Vermont (16th) are also ranked in the top 20 states for long-acting/extended-release prescribing. All six New England states also have above-average rates of high-dose opioid prescribing, and all but Vermont have above-average prescribing rates for benzodiazepines—psychoactive sedatives commonly abused along with opiates, drastically increasing overdose risk.
{kind=link}
Rachel Bissett/Federal Reserve Bank of Boston
Saving Lives and Communities
Although physicians are aware of the highly addictive nature of opioids and are cognizant of the overdose risk, they also know that if they cut patients off from these highly addictive narcotics, some are likely to turn to heroin, which, thanks to increased distribution from Mexico, has become easily accessible and incredibly cheap: heroin is now cheaper than a pack of cigarettes or a six-pack of beer in most parts of the United States.13
Although increasing first-responder and community access to naloxone (a drug that counteracts the effects of an opioid overdose) has potential to reduce overdoses, and increased use of medication-assisted treatments like buprenorphine holds potential for treating opioid dependence, preventing initiation is the key to turning the tide on the opiate abuse and overdose epidemic. About 60 percent of current heroin users report first using heroin between the ages of 17 and 25,14 suggesting that those are the years to target. Different strategies will work better in different communities, but general prevention strategies include more comprehensive physician training in pain management and addiction, moving physicians toward safer prescribing practices, and better parent and youth education on the risks of opioid use for minor injuries. Finally, given high rates of abuse and overdose in communities that have long suffered from employment restructuring and economic decline, comprehensive job-growth strategies that emphasize secure employment with livable wages for individuals all along the educational gradient are likely to have the most significant long-term and sustainable impacts in New England and elsewhere.
Articles may be reprinted if Communities & Banking and the author are credited and the following disclaimer is used: "The views expressed are not necessarily those of the Federal Reserve Bank of Boston or the Federal Reserve System. Information about organizations and upcoming events is strictly informational and not an endorsement."

 About the Authors
About the Authors
Shannon M. Monnat,
Pennsylvania State University
Shannon M. Monnat is an assistant professor of rural sociology, demography, and sociology at Pennsylvania State University.
Email: smm67@psu.edu
Endnotes
- “Multiple Cause of Death Data,” Centers for Disease Control and Prevention, 2016, http://wonder.cdc.gov/mcd.html.
- Ibid.
- Shannon Monnat and Khary K. Rigg, “Rural Adolescents Are More Likely Than Their Urban Peers to Abuse Prescription Painkillers” (Carsey Research National Fact Sheet No. 32, Carsey School of Public Policy, University of New Hampshire, 2015).
- Shannon Monnat and Khary K. Rigg, “Examining Rural/Urban Differences in Prescription Opioid Misuse Among US Adolescents,” Journal of Rural Health 32, no. 2 (2016):204–18.
- “National Survey on Drug Use and Health (NSDUH) Series,” Substance Abuse and Mental Health Services Administration, http://www.samhsa.gov/data/population-data-nsduh.
- Monnat and Rigg, “Rural Adolescents Are More Likely Than Their Urban Peers to Abuse Prescription Painkillers.”
- Sam Quinones, Dreamland: The True Tale of America’s Opiate Epidemic (London and New York: Bloomsbury, 2015).
- “Trends in Nonmedical Use of Prescription Pain Relievers: 2002 to 2007” (report, National Survey on Drug Use and Health, Rockville, MD, 2009), http://media.samhsa.gov/data/2k9/painRelievers/nonmedicalTrends.htm.
- “Multiple Cause of Death Data.”
- Ibid.
- “National Survey on Drug Use and Health (NSDUH) Series.”
- L.J. Paulozzi, K.A. Mack, and J.M. Hockenberry, “Vital Signs: Variation Among States in Prescribing of Opioid Pain Relievers and Benzodiazepines – United States, 2012,” Morbidity and Mortality Weekly Report 63, no. 26 (2014):563–68.
- L. Bernstein, “Why a Bag of Heroin Costs Less Than a Pack of Cigarettes,” Washington Post, August 27, 2015.
- “National Survey on Drug Use and Health (NSDUH) Series.
Resources
Site Topics
Keywords
- Opioids ,
- New England